

Post-acute Care Solutions for Effective Care Transitions
We help transition members to the right site of care following acute patient stays and coordinate care transitions with member families and clinical teams.
![]()
![]()
![]()
![]()


We work with you to provide quality patient care
Members deserve to get the right care at the right time. As part of Optum® Home and Community offerings, naviHealth Post-acute Care Solutions partners with you to make sure members get to live more fulfilling lives.
We work with health plans, hospitals, health systems, post-acute providers, skilled nursing facilities, physician groups and Accountable Care Organizations (ACOs). Together we:
- Drive better post-care outcomes
- Simplify and improve care transitions to meet clinical and non-clinical member needs
- Close gaps resulting from social determinants of health (SDOH) and health-related social needs
We support your effective care resource management
Our post-acute care management solutions help you:
- Ensure proper placement – We deploy in-market clinical care coordinators to work closely with patients.
- Engage members – We coordinate care transitions to align resources. We also connect members to benefits provided by health plans as well as community programs.
- Identify gaps in care – We partner with both clinical and community resources to help close any gaps in care for the member. This helps lower readmission risks, increase patient satisfaction and improve Support, Transform, Achieve and Results (STAR) measures.
- Plan for safe discharge – Early discharge planning is key. We start by working with local, in-market providers to make sure they get the right clinical information and fully understand a member’s demographics, functional levels and other unique needs.

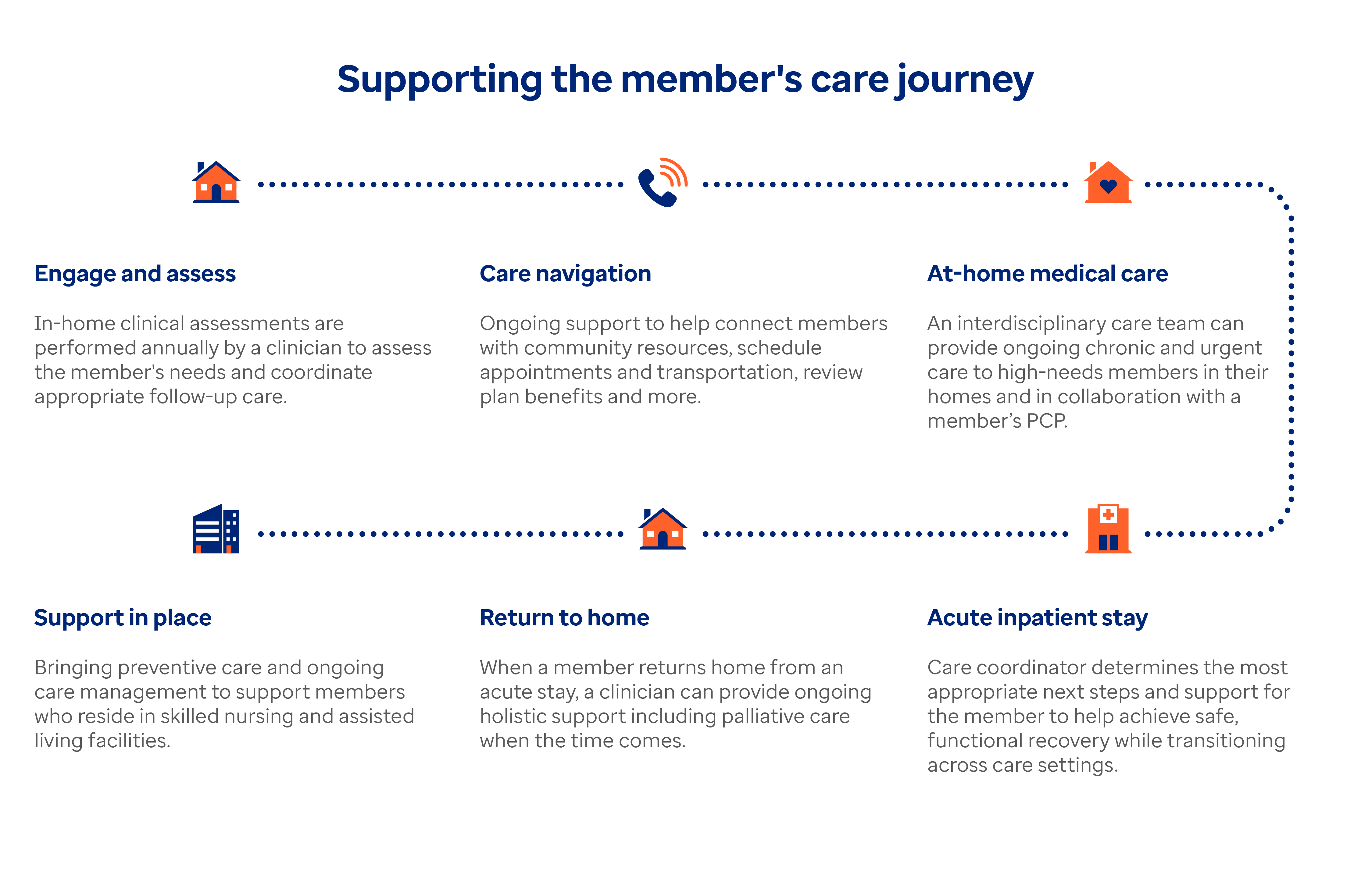
Infographic shows a chart with the title “Supporting the member’s care journey.” The chart starts with the first heading Engage and Assess: In-home clinical assessments are performed annually by a clinician to asses the member’s needs and coordinate appropriate follow-up care. The next heading is Care navigation: Ongoing support to help connect members with community resources, schedule appointments and transportation, review plan benefits and more. The next heading is At-home medical care: An interdisciplinary care team can provide ongoing chronic and urgent care to high-needs members in their homes and in collaboration with a member’s PCP. The next heading is Acute patient stay: Care coordinator determines the most appropriate next steps and support for the member to help achieve safe, functional recovery while transitioning across care settings. The next heading is Return to home: When a member returns home from an acute stay, a clinician can provide ongoing holistic support including palliative care when the time comes. The next heading is Support in place: Bringing preventive care and ongoing care management to support members who reside in skilled nursing and assisted living facilities.